
Phase 1 – Construction and evaluation of the TRL 5 prototype (2025)
This section presents the main results of the activities carried out within Stage 1 – Construction and evaluation of the TRL 5 prototype of the TraViMo project.
Results:
(1) State of the art report regarding relevant technologies
During Stage 1, taking into account the rapid technological progress, a series of studies were carried out:
- Detailed study of the current state of EEG-based motor imagery evaluation
- Detailed study of hardware equipment for EEG
- Detailed study of existing OpenVibe resources relevant to the project
- Detailed study of the current state of VR for relaxation and concentration training
(2) The User Requirements Document (URD)
The URD was developed based on the detailed requirements expressed by all consortium members, taking into account the vision established in the project proposal and the results of the conducted studies.
The URD has detailed the requirements and specifications for:
- the new capabilities of the web platform
- extension of activity management
- extension of VR device management
- extension of session management
- extension of user account management
- improvements to the BCI system
- the new capabilities of the VR system
- adaptation of the game-based exercise named ‘rocket’
- updating the system for ‘Meta Quest 3’ devices
- creation of a multilingual data management system
- unification of VR application versions
- visual improvements
- the new game-based exercises used with the early-stage neuromotor recovery system
- the game-based exercise named ‘feeding the animals’
- the game-based exercise named ‘the letters’
- the game-based exercise named ‘jumping over obstacles’
- the relaxation and concentration environments
- the ‘nature’ environments
- the ‘birds’ environment
- the ‘plants’ environment
- the ‘ball tracking’ environment
- the ‘WateRo’ environment
- the ‘nature’ environments
(3) Acquisition of AI training data
Within this activity, the procedure and infrastructure for acquiring the different types of data required for AI training were established, as well as the actual acquisition of EEG data.
Procedure and infrastructure for acquiring AI training data
- EEG acquisition procedure: the protocol represents a repetitive cycle of 40 trials (full session), each trial having standardized, time-synchronized steps. The goal is to obtain labeled EEG segments (background/attention, left-hand motor imagery, right-hand motor imagery), required for training AI models
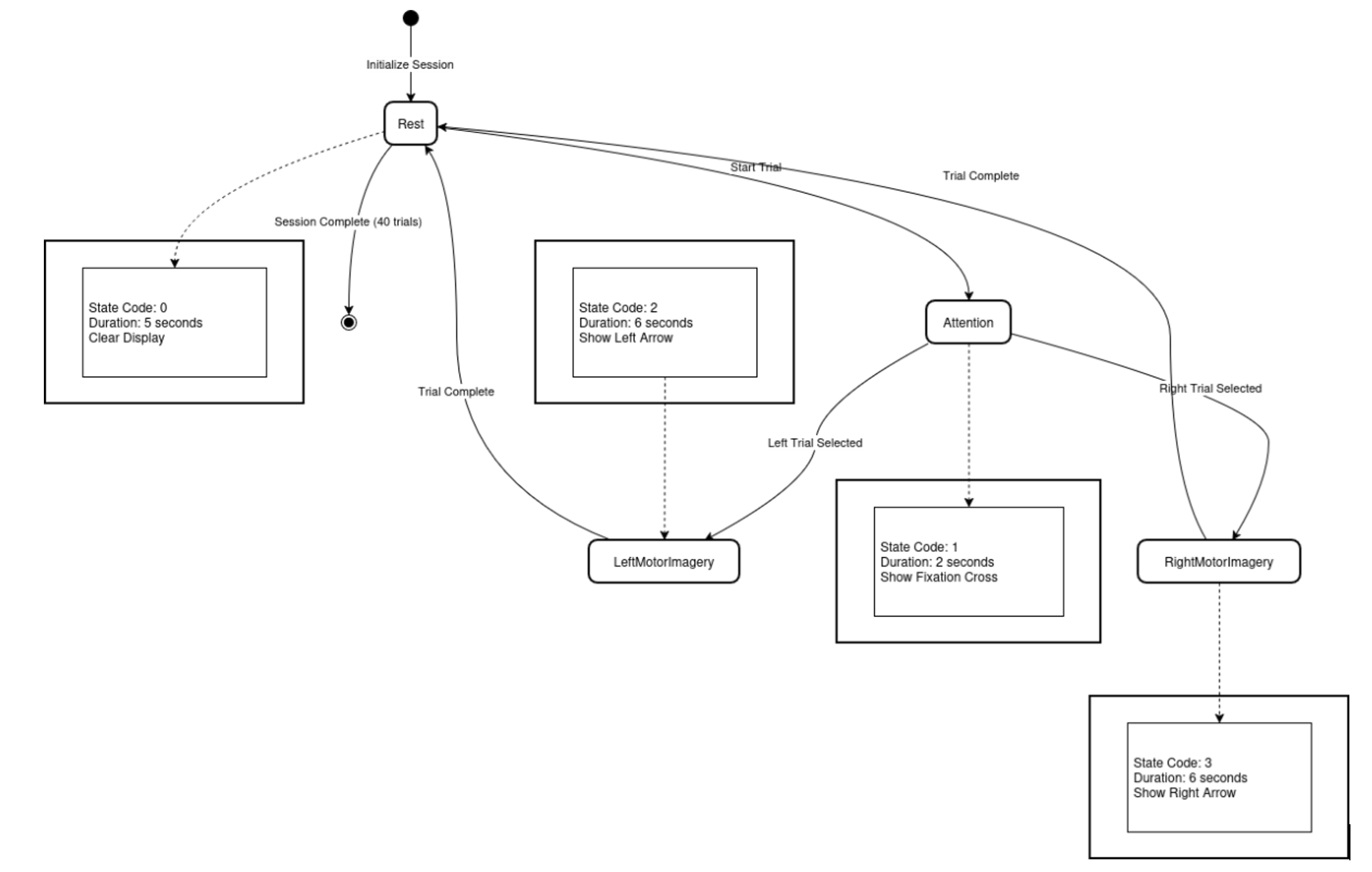
Fig. 1: States in which the acquisition system operates (state machine)
- FES stimulation procedure (Functional Electrical Stimulation): the proposed system includes four essential components that interact with each other to perform functional electrical stimulation. Two plugins were developed on the OpenViBE platform to allow control of the stimulation device
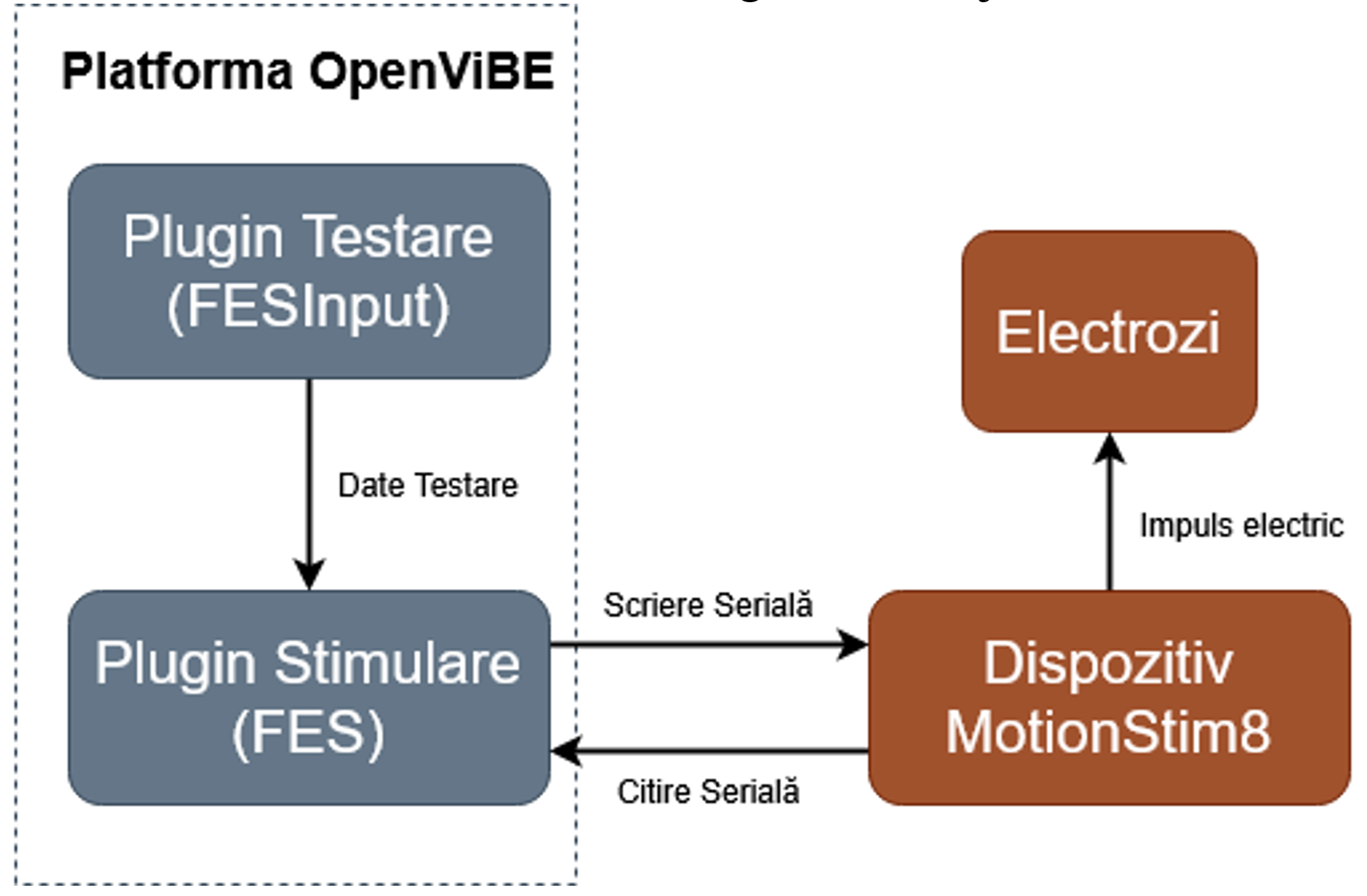
Fig. 2: System architecture diagram
- Proprioceptive stimulation: numerous recent studies support the integration of proprioceptive feedback into rehabilitation protocols, emphasizing the beneficial effects of focal muscle vibration (FMV) on upper-limb coordination and overall functionality. These effects become even more evident when stimulation is integrated into complex rehabilitation systems that include virtual reality (VR), brain-computer interfaces (BCI), and haptic feedback. Consequently, integrating a proprioceptive stimulation device into the TraViMo system was pursued.
EEG data acquisition for AI model training
- subject cohort and dataset characterization: a study was conducted based on the analysis of an extensive and complex dataset, obtained from a cohort of 19 patients who had suffered a stroke; in total, more than 450 cumulative recording sessions were collected and validated from the 19 subjects. The analysis of the session distribution per patient reveals a significant variation, reflecting real-world adherence to treatment in the clinical environment; the dataset included a variety of neurophysiological profiles, from patients with a preserved ability to generate clear sensorimotor rhythms (subjects with high “BCI literacy”), to patients with attenuated or distorted signals, enabling a comprehensive evaluation of the performance of the proposed system
- hardware infrastructure and electrode configuration: acquisition of bioelectric signals was performed using the BCI2000 platform, a reference system in BCI research due to its flexibility and reliability in synchronizing stimuli with data acquisition. The system was equipped with a high-density EEG cap with 64 active channels. The use of wet electrodes was preferred over dry electrodes to ensure optimal impedance at the scalp–electrode interface and to maximize the signal-to-noise ratio-critical for detecting the weak potentials associated with motor imagery
- experimental protocol and task paradigm: the experimental protocol was designed to maximize the clarity of the neurophysiological response while minimizing cognitive artifacts and patient fatigue. The paradigm used is a classical “Left Hand vs. Right Hand Motor Imagery” task, a binary task that exploits the contralateral lateralization of Mu-rhythm desynchronization
- the calibration challenge and the proposed approach: the experimental methodology was rigorously designed to generate a high-quality, clinically relevant dataset, enabling an in-depth investigation of the current capabilities of artificial intelligence algorithms in decoding human motor intention.
(4) Report and integrated BCI AI modules
The technical report corresponding to this activity is logically organized into three major chapters, each addressing an essential dimension of the TraViMo system—from source code implementation to neural network training and clinical validation.
Development of the new and independent BCI module
The first part details the software engineering effort dedicated to creating an autonomous BCI component. The work began with a critical analysis of the limitations of earlier versions, which depended on heavy external software ecosystems.
- Dual Architecture: the report describes the parallel investigation of two implementation paths: a high-performance C++ variant (integrating the OpenViBE core for direct memory and thread management) and a flexible Python variant (based on the MNE library, enabling rapid integration of AI models)
- Optimized Protocol: the design of the stimulation protocol is presented, specifically calibrated for the neuropsychology of post-stroke patients. The temporal sequence was refined to include cognitive relaxation intervals (3–4 seconds), clear visual cues (2 seconds), and extended motor imagery windows (4–5 seconds), maximizing the likelihood of capturing desynchronization of sensorimotor rhythms
- Interface and Feedback: the implementation of the graphical user interface (UI) is described, which closes the control loop by providing the patient with real-time visual feedback-a crucial element for Hebbian learning and neuroplasticity.
AI model preparation and infrastructure
This part represents the scientific “engine” of the report, providing a comprehensive analysis of signal-processing methods.
- Advanced Preprocessing: the data-cleaning workflow is detailed, including spectral filtering in the 8–30 Hz band (Mu/Beta rhythms) and the use of Independent Component Analysis (ICA) for the automatic removal of ocular and muscular artifacts, retaining only components of neural origin
- Classical and Geometric Algorithms: the implemented reference methods are presented, from Common Spatial Pattern (CSP) filtering combined with Linear Discriminant Analysis (LDA), to advanced Riemannian Geometry methods (Tangent Space Mapping), which have proven extremely robust to signal amplitude variations
- The Deep Learning Revolution: deep neural architectures are described, including analyses of Convolutional Neural Networks (EEGNet, ShallowConvNet) optimized for low-data scenarios, Recurrent Networks (LSTM/GRU) for temporal dynamics, and, for the first time, the adaptation of Transformer-based models and Foundation Models (CBraMod), trained on GPU clusters to extract universal representations of brain activity.
Development of the autocalibration module and results
The final part synthesizes the operational innovation of the project: overcoming the calibration-time barrier.
- Two-Stage Solution: the hybrid architecture is presented, enabling patient stratification: a rapid 8-minute screening for validating BCI capability and a precision module for long-term therapy
- Rigorous Validation: the report details the Leave-One-Session-Out (LOOSO) and Leave-One-Subject-Out (LOSO) testing protocols, applied to the cohort of 19 patients
- Key Results: the data show that the use of Riemannian Geometry ensures an average accuracy of 77.4% in the persistence scenario (intra-subject), eliminating the need for daily recalibration. Furthermore, the use of foundation models (CBraMod) enabled an accuracy of 71.5% in a “Zero-Shot” regime (with no prior calibration), validating the feasibility of a universal “Plug-and-Play” BCI system and confirming the achievement of TRL 5.
(5) Report and integrated VR modules
Within this activity, based on the URD document, the new functionalities / extensions of the TraViMo system were developed and implemented for the web platform / VR environments.
Improvements (refinements / extensions) required for the current modules
- Improvement of the web panel for assisting recovery sessions: within the current project, multiple improvements were made to the Web panel from the TRAVEE project
- Extension of activity management: additional information/functionality for the compatibility of an activity with the HDC application, the usage context in which an activity can be used, the type of an activity, displaying a window with additional information, searching for an activity by name and type, ordering and managing activities
- Extension of VR device management: additional information/functionality for the model of VR devices in the system, ordering and managing VR devices
- Extension of session management: additional information/functionality for a mechanism of automatically closing sessions that remain open in the system, managing the creation of work sessions
- Extension of user account management: additional information/functionality for the creation date of user accounts, automatic ordering by creation date, the option to view the text entered in the password field
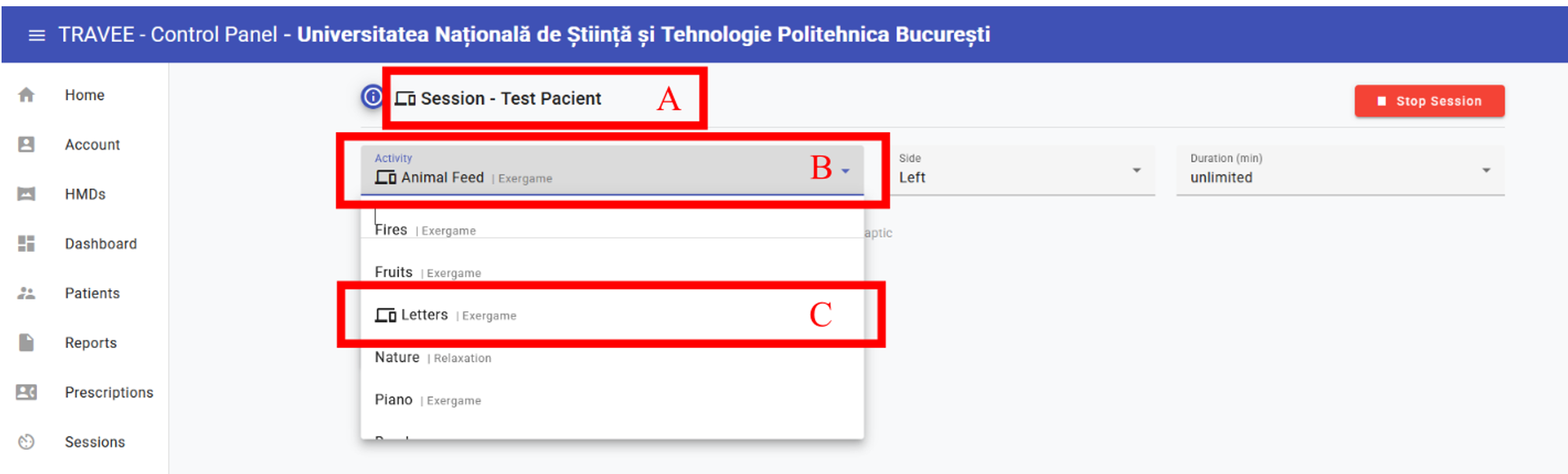
Fig. 3: Screenshot from the web platform interface for managing a session
- New capabilities of the VR system: within the current project, multiple improvements were made to the VR application from the TRAVEE project.
- Adaptation of the game-based exercise named “Rocket”: in the TRAVEE project, the “Rocket” game-based exercise was used for conducting early-stage neuromotor recovery sessions. During the use of the exercise, multiple improvements were identified and implemented to increase its quality. Most observations that led to modifications of the “Rocket” game-based exercise were due to using the system with early-recovery patients who did not have strong cognitive function, requiring adaptations to the exercise for proper execution with these patients

Fig. 4: Screenshot from the VR application showing the “Rocket” exercise, where the patient’s hands were displayed in blue to ensure visibility for a wide range of patients
-
- Updating the system for “Meta Quest 3” devices: the VR application was updated so it can be used with “Meta Quest 3” devices
- Creation of a multilingual data management system: a complex system was created for managing activity-configuration parameters in multiple languages. This system was implemented in all software components: the Web panel, the VR application, and the server
- Unification of VR application versions: in the TRAVEE project, two versions of the VR application were developed in parallel—one for neuromotor recovery sessions in clinical settings and another for recovery sessions at home. This decision was not made for design reasons, but to ensure that the two versions would not suffer from technical issues during recovery sessions. In Stage 1 of the current project, the development team decided to unify the two VR versions to simplify the development process
- Visual improvements: multiple visual improvements were implemented in the VR application.
Development of gamified VR exercises for neurofeedback with visual movement augmentation
A total of 3 new game-based exercises were created for use in early-stage neuromotor recovery sessions. It is important to note that the development team aimed to maintain compatibility of these exercises for use in advanced-stage recovery sessions as well
- Game-based exercise named “Feeding the Animals”: the goal of the exercise is to increase patient engagement in early neuromotor recovery sessions through interaction with virtual animals. Before each signal emitted by the recovery system, a puppy appears from behind the patient and positions itself in front of them. When the patient raises their palm, a piece of food is generated and thrown toward the puppy, which moves to retrieve it and then leaves the field of view. Afterwards, another puppy takes its place. If the patient does not raise their palm, the puppy remains in front of them until the next command. The system allows multiple types of puppies or other animals to offer visual variety and create a stimulating and pleasant environment, encouraging active participation in the recovery process
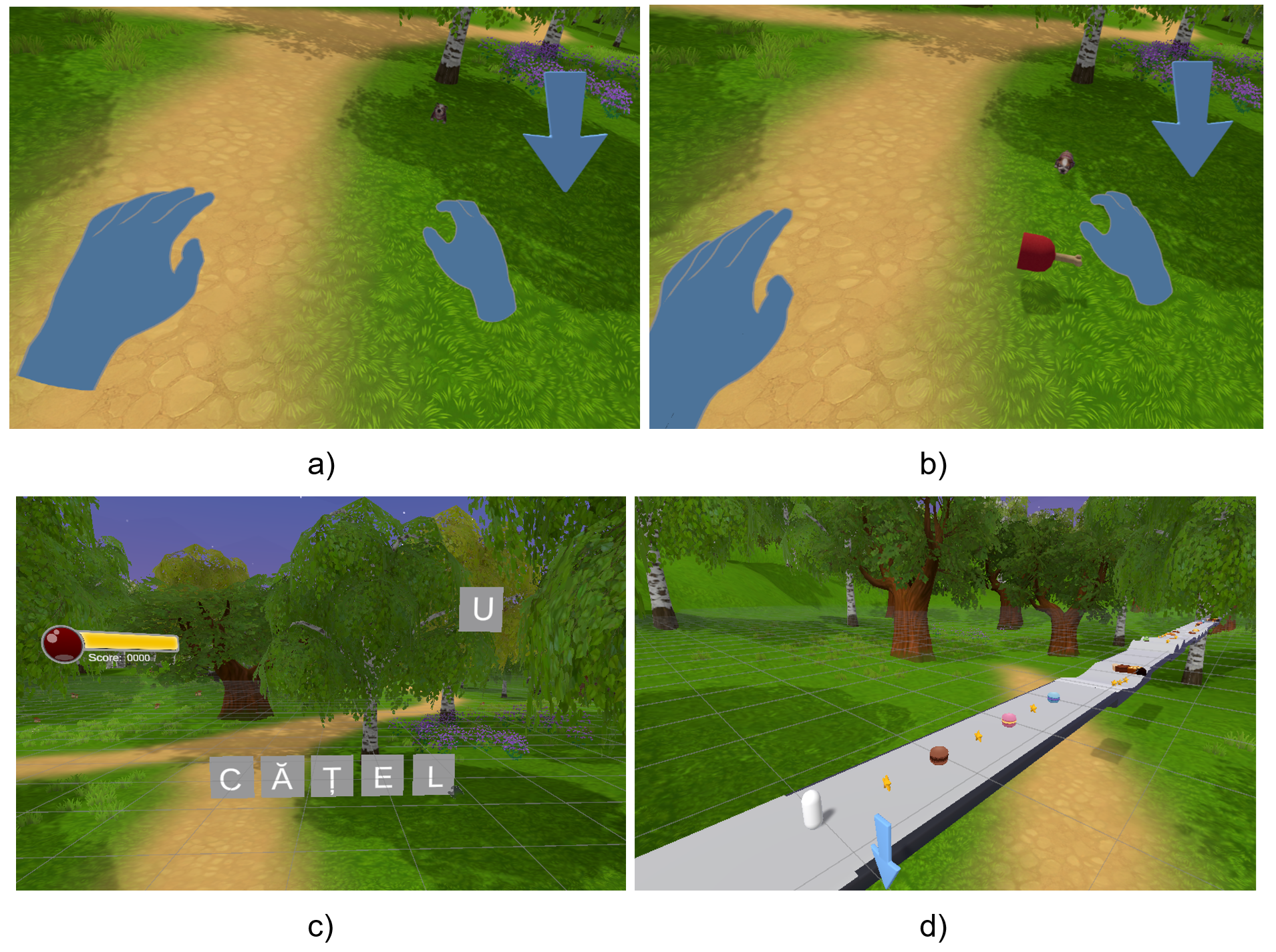
Fig. 5: Screenshots from the game-based exercises used during early neuromotor recovery sessions. The screenshots labeled (a) and (b) are from the “Feeding the Animals” exercise. The screenshot labeled (c) is from the “Letters” exercise. The screenshot labeled (d) is from the “Jumping Over Obstacles” exercise.
- Game-based exercise named “The Letters”: the exercise aims to complete a phrase displayed in the virtual environment, which is different in each session. A few seconds before the signal from the early neuromotor recovery system, a letter moves from left to right and stops in front of the patient. Such a scenario can be seen in the screenshot labeled (c) in the figure above. The letter “U” appears in the scene. Raising the palm at the indicated moment makes the letter move—through a dedicated animation—to the correct position in the displayed phrase
- Game-based exercise named “Jumping Over Obstacles”: this exercise proposes that the patient indirectly control a runner viewed from above, depicted as a simplified geometric shape for easier understanding. This scene appears in the screenshot labeled (d) in the above figure. In front of the patient, the race track is displayed, populated with cupcake-shaped obstacles. A few seconds before the signal from the early neuromotor recovery system, an obstacle appears in front of the runner, causing it to stop. If the patient raises their palm at the required moment, the runner jumps over the obstacle and continues the race. In the absence of this action, the runner waits until the next command. The exercise allows multiple types of obstacles to diversify the visual experience and increase patient motivation and engagement during the recovery session.
Creation of VR environments for mental relaxation and concentration training
- “Nature” environments: these environments include static and dynamic natural elements designed to induce a state of relaxation in patients. The “Nature” environments contain the following: procedurally generated terrain and river, various plants (trees, animated grass influenced by wind, plants with stems, branches, leaves, and flowers that grow over time following an algorithm), a modifiable skybox (indicating different times of day/night), natural spatial sounds that create a relaxing sensation. There are three types of “Nature” environments: “Birds,” “Plants,” and “Full.” In the “Birds” environment, the user follows a flock of birds in the sky (performing the required action triggers visual and auditory feedback). In the “Plants” environment, the user observes the growth of a plant (receiving visual feedback for the growth of its stem, branches, leaves, and flowers). In the “Full” environment, the user has no specific task, but can observe various elements (plants, flying birds, ducks, sheep, a dog). The figure below shows screenshots from the “Nature” environments
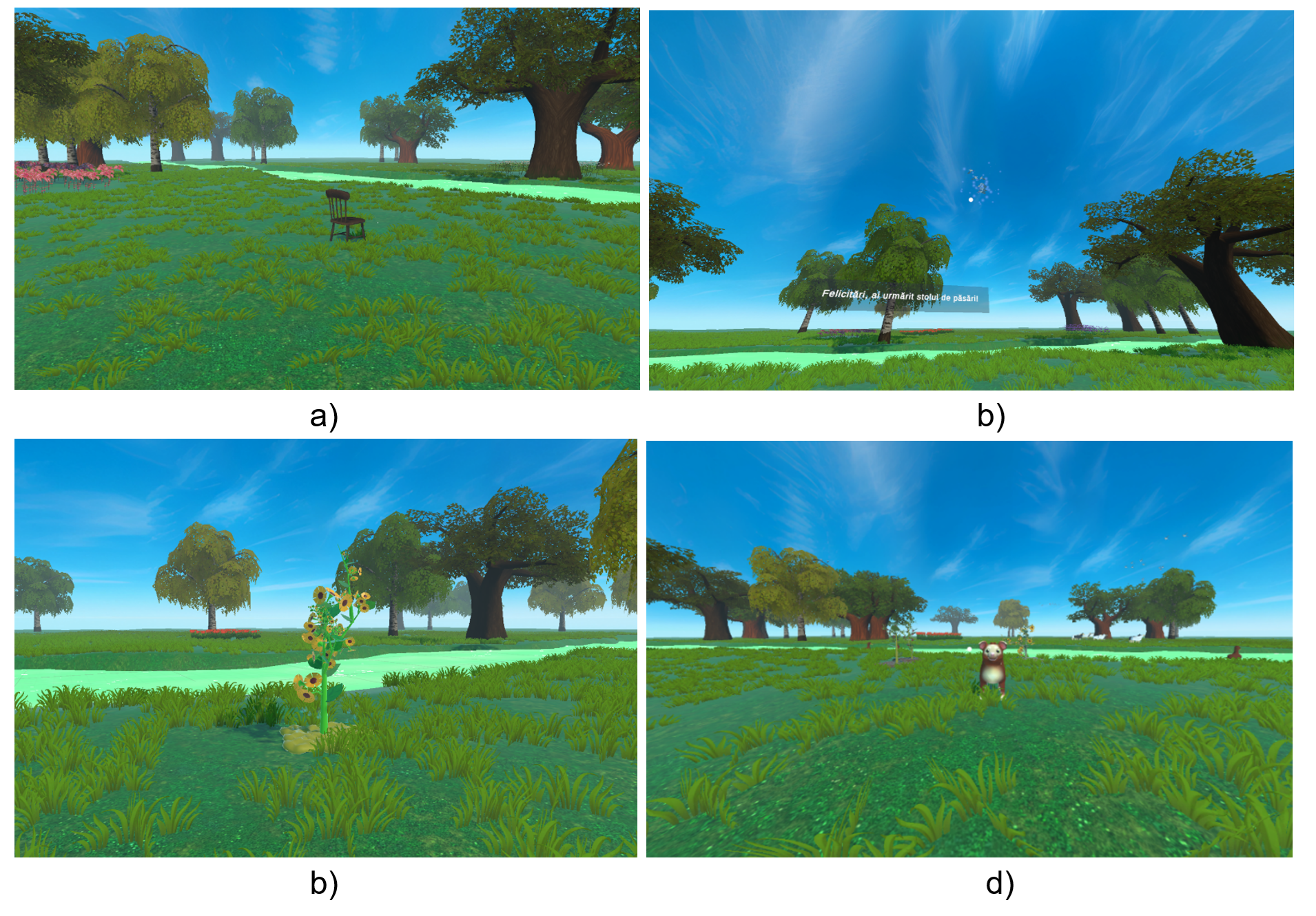
Fig. 6: General scene from the “Nature” environments (a); scene with a congratulatory message from the “Birds” environment (b); scene with a fully developed plant in the “Plants” environment (c); scene showing the puppy and ducks in the “Full” environment (d)
- “Ball Tracking” environment: this VR environment is designed to train patients’ visual attention and ability to concentrate, within a minimalist setting free of distracting stimuli. The user is placed in a simple, calming space where a ball moves continuously along a trajectory chosen by the therapist. Interaction is performed through a targeting cursor placed at the center of the screen. The goal is for the patient to keep the cursor on the ball, at which point the ball changes color from turquoise to purple, signaling correct tracking. The environment includes two modes: exercise mode, where the cursor is active and focus time is measured; and spectator mode, where patients simply observe the ball’s movement without being evaluated. The figure below shows screenshots from the “Ball Tracking” environment
Fig. 7: “Ball Tracking” relaxation-concentration environment: scenario in which the user does not track the ball (a); scenario in which the user successfully tracks the ball (b)
- “WateRO” relaxation environment: The WateRO application is an interactive virtual environment that allows users to explore real locations in Romania related to the country’s water resources. Initially designed as a standalone VR application at the National University of Science and Technology POLITEHNICA Bucharest, WateRO was later integrated into the TRAVEE platform, where it serves as a therapeutic relaxation environment. The user can navigate a 3D map of Romania, select points of interest, and view 360° footage recorded on-site, offering an immersive, relaxing, and educational experience. The figure below shows screenshots from the “WateRO” relaxation environment.
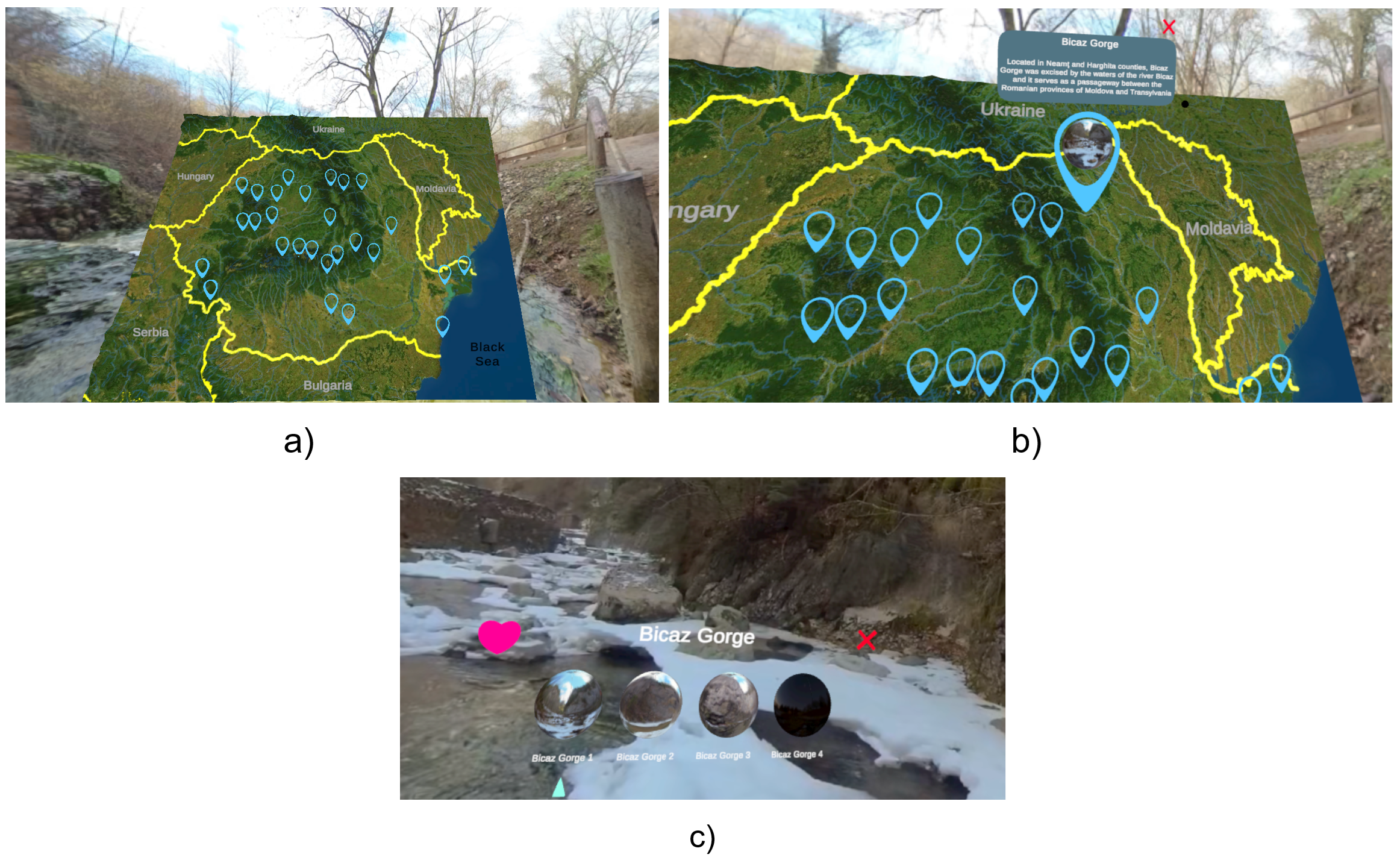
Fig. 8: “WateRO” relaxation environment: map of Romania (a); selecting a pin on the map (b); visiting a location and the menu for selecting another video (c)
(6) Report on clinical piloting of the new modules
Clinical piloting focused on the new BCI / AI components
The objective of this clinical piloting is: evaluation of the clinical feasibility of using an MI-BCI system with VR feedback in stroke patients (session completion rate, tolerability, effective usage time, major technical issues).
The developed BCI system represents an improvement over previous versions, as it no longer depends on restrictive external software ecosystems and integrates artificial intelligence components calibrated for EEG signals specific to stroke patients. The BCI component, in its current form, combines EEG neuroimaging with advanced machine learning algorithms, and this report narratively explores the possibility of its clinical validation.
- the BCI system used is non-invasive, with 8–32 channels placed predominantly over the motor and premotor areas (e.g., C3, C4, Cz and nearby sites), using an EEG cap with wet electrodes. A standard motor imagery protocol is used—imagining extension of the affected hand—with the following sequence:
relaxation period (2–3 s) - presentation of a visual cue (arrow, avatar) (1–2 s)
- sustained motor imagery phase (4–6 s)
- contingent feedback (visual in VR).
All patients were evaluated according to the assessment standard used in the clinic. Inclusion and exclusion criteria established prior to the start of the study were applied.
All patients who met the inclusion criteria were enrolled in the adapted and individualized conventional rehabilitation program applied in the clinic. At the same time, the TraViMo program corresponding to each patient’s phase of medical rehabilitation was applied. Each patient participated in 1–12 training sessions with the personalized TraViMo program (for the early rehabilitation phase and for the second phase of medical rehabilitation).
Clinical piloting focused on the new VR components
The objective of the clinical piloting was to evaluate the three VR relaxation environments integrated into the TRAVEE platform (Nature, Ball Tracking, and WateRO) from the perspective of users diagnosed with stroke (AVC). Aspects such as enjoyment of the experience, ease of use, level of engagement, visual and physical comfort were analyzed. In total, 53 questionnaires were completed by 14 patients, each testing one or more environments.
The piloting took place over three days, each day including both new patients and returning patients. Depending on clinical condition and availability, participants tested between 1 and 3 VR environments, with most managing to experience all three types.
Each environment was evaluated using a 12-item questionnaire, the first 11 questions being rated from 1 to 5 (where 1 = minimum, 5 = maximum), and the last question being open-ended. The questions assessed: enjoyment of the environment, intuitiveness, engagement, fatigue, dizziness, anxiety, physical discomfort, image clarity, understanding of instructions, and intention to reuse.
The 14 patients included in the pilot were diagnosed with stroke and presented varying levels of neurological impairment, mobility, and technological experience. The distribution of time since stroke was:
- 57% in the first three months post-stroke
- 14% between 3 and 12 months
- 3 patients between 2 and 6 years after stroke
Most had never used VR before, which made it possible to evaluate the authenticity of a first interaction with an immersive system. Five patients had previous VR experience, including with earlier versions of the TRAVEE system. Thus, the piloting covered both completely new users and familiar users, reflecting the general accessibility of the environments.
Analysis of the 53 questionnaires shows exceptional clinical acceptance of all VR environments. Average scores are consistent and very high on positive questionnaire items, ranging between 4.70 and 4.96. Percentage-wise, between 90% and 98% of responses are rated with the maximum score (5), confirming that the environments are intuitive, accessible, clearly visible, and pleasant. Reported adverse symptoms were almost nonexistent. Regarding questions evaluating patient discomfort, responses showed extremely low averages (between 1.04 and 1.13). Between 94% and 98% of patients selected “1 – not at all.” No patient assigned the maximum score to negative symptoms. This confirms that the VR environments are safe, gentle, well-calibrated, and suitable even for patients in the first months after stroke—a group vulnerable to fatigue and visual overload.
(7) Writing 5 scientific articles
Reducing Calibration Time in EEG Motor Imagery BCI: A TwoStage Approach for Clinical Deployment
Cristian-Stelian Grecu, Nicolae-Alexandru Botezatu and Robert-Gabriel Lupu
Design and validation of a portable proprioceptive stimulator for upper limb rehabilitation
Nicolae Alexandru Botezatu, Valentin Gîscă, Paul Corneliu Herghelegiu and Robert Gabriel Lupu
Immersive Virtual Reality for Stroke Rehabilitation: Linking Clinical and Digital Measures of Motor Recovery — A Pilot Study
Livia-Alexandra Ion, Miruna Ioana Săndulescu, Claudia-Gabriela Potcovaru, Daniela Poenaru, Andrei Doru Comișel , Ștefan Ștefureac, Andrei Cristian Lambru, Alin Moldoveanu, Ana Magdalena Anghel, Delia Cinteză
Designs of VR Environments for Relaxation and Focus – A Systematic Review
Silviu Stăncioiu, Anca Morar, Alin Moldoveanu, Cristian Lambru, Ana Magdalena Anghel
Stroke diagnosis VR trainer for neurology residents
Awss Zidan, Ayham Boucher, Emil Dragan, Anca Morar, Alin Moldoveanu
(8) Development of the TraViMo project website